
A new antibody pattern called anti-DFS70 can help determine which patients who test ANA-positive have a low risk of developing an autoimmune rheumatic condition
Finding a patient has antinuclear antibodies can be confusing. Does it signal underlying autoimmune rheumatic disease or is it an incidental finding? Testing for little known DFS70 antibody pattern can help.
Antinuclear antibody (ANA) testing has long been the first-line test to help identify autoimmune rheumatic disease, and more importantly helps determine who doesn’t have autoimmune rheumatic disease.
Patients who have a negative ANA test can be 99% sure that they don’t have lupus (SLE) and 95% sure that they don’t have other diseases such as scleroderma, Sjögren syndrome and type 1 autoimmune hepatitis.
But a positive ANA test is less predictive, as up to 20% of healthy patients are also ANA positive.
Over the last decade, a new antibody pattern called anti-DFS70 has been proven useful for determining which ANA-positive patients have a low risk of developing an autoimmune rheumatic condition.
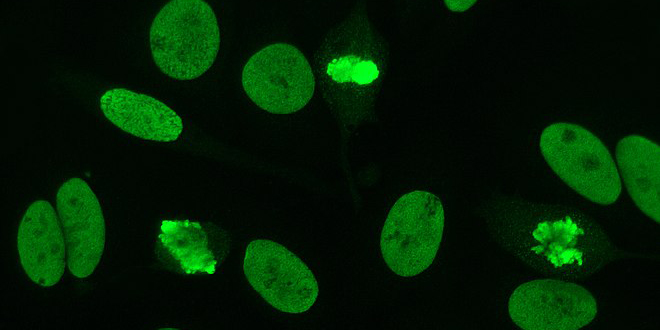
ANAs bind to a variety of distinct cell nuclear molecules. Different ANA patterns can be detected using a fluorescent label that binds to the fixed, bound autoantibodies.
Dense fine speckled ANAs (anti-DFS70) are named after their very distinct pattern. This ANA type is almost never seen in patients with rheumatic disease, so patients who are ANA positive and anti-DFS70 positive are highly unlikely to develop symptoms.
Anti-DFS70 is only found in around 5 to 10% of ANA-positive patients, but it is a relatively straightforward pathology test that can help reassure patients that their ANA-positive result is of little, if any, significance.
“If you order an ANA and if you find the anti-DFS70 antibody is positive, then you normally don’t need to refer onwards to a rheumatologist – so, you can save that referral,” Dr Pravin Hissaria, a pathologist and rheumatologist based in Adelaide, advised GPs.
However a potential barrier to ordering an anti-DFS70 antibody test in Australia was that only a afew pathology labs ran the necessary confirmatory tests, such as an immunoblot, said Dr Hissaria.
GPs probably needed to check whether their lab was confirming their anti-DFS70 antibody test result, he advised GPs.
“You have to be confident about the lab,” he said. “You have to be confident about the lab.”
Dr Hissaria co-authored a paper on anti-DFS70 testing in the MJA this month along with Sydney-based immunologist Dr Karl Baumgart.
Currently, the test is not covered by Medicare, which is “one of those little cracks in the healthcare system”, Dr Baumgart said. But pathology labs usually only charge a small fee, if anything, for the additional test so it is still worth asking for it.
“Some people have a low positive ANA with negative other tests (ENA, dsDNA, Chromatin) and what follow-up they should have is determined by both clinical and lab features,” Dr Baumgart said. “A dense fine speckled pattern excuses them from longer-term follow up. A Medicare rebate for confirming this pattern could be very cost-effective as well as good clinical medicine and public health practice.”
Dr David Gillis, an immunologist based in Queensland, said anti-DFS70 antibody testing had some role in excluding rheumatic disease but that blood test results had to be taken in context.
If someone had obvious rheumatic disease, antibodies took a secondary role, he said. And sometimes another ANA pattern might have more clinical relevance than the anti-DFS70 antibody pattern.
